55 YEAR FEMALE K/C/O OF DM SINCE 3 YEARS ON OHAS WITH C/O GIDDINESS
This is online E-blog, to discuss our patient de-identified health data shared after taking her guardian's signed informed consent.
Here we discuss our individual patient problems through series of inputs from available global online community of experts with an aim to solve the patients clinical problem with current best evidence based input.
This E-blog also reflects my patient's centred online learning portfolio.
I have been given this case to solve in an attempt to understand the topic of "Patient Clinical Data Analysis" to develop my competency in reading and comprehending clinical data including history, clinical findings, investigations and come up with a diagnosis and treatment plan.
Case History and Clinical Findings:
55 YEAR FEMALE K/C/O OF DM SINCE 3 YEARS ON OHAS
PATIENT CAME WITH C/O GIDDINESS SINCE YESTERDAY MORNING FOLLOWING
EXOPOSURE TO HEAT AND WENT TO RMP -SBP WAS 70MMHG AND 10 NS GIVEN -AND SHE
DEVELOPED FACIAL PUFFINESS ,PEDAL EDEMA.
C/O LOOSE STOOLS SINCE TODAY 5-6 EPISODES
NO H/O VOMITINGS ,PAIN ABDOMEN
C/O BOWEL AND URINARY INCONTINENCE 4 TIMES SINCE TODAY MORNING .
NO C/O SEIZURES ,HEADACHE.
SOB GRADE 4 SINCE @ 4PM TODAY , PEDAL EDEMA SINCE 1 DAY
UNRESPONSIVE SINCE 15 MINUTES
AT OUTSIDE HOSPITAL ; SERUM CREATININE -2.1, PH-6.7
K/C/O DM SINCE 3 YEARS
VITALS
TEMP-98.6F
PR-110BPM
BP-140/100MMHG
RR-26CPM
SPO2- 29% @ ROOM AIR
GRBS-331MG/DL
NO PALLOR/ICTERUS/CLUBBING/CYANOSIS/LYMPHADENOPATHY
EDEMA PRESENT
CVS-S1,S2 HEARD
RS-BAE PRESENT,DIFFUSE WHEEZE PRESENT
P/A- BOWEL SOUNDS PRESENT
CNS-UNESPONSIVE
GCS-E1V1M1
SPEECH-NO RESPONSE
Diagnosis
IMMEDIATE CAUSE OF DEATH : SEVERE METABOLIC ACIDOSIS WITH TYPE 2 RESPIRATORY
FAILURE
ANTECEDENT CAUSE OF DEATH : ACUTE GASTROENTERITIS WITH AKI ,MIXED ACIDOSIS ,?
HYPERCAPNIC ENCEPHALOPATHY
TREATMENT:
1]INJ LASIX 40MG IV STAT
2]INJ NAHCO3 50 MEQ IV STAT-> 100MEQ +100ML NS OVER 1 HOUR
3]INJ HUMAN ACTRAPID 3C IV STAT
4]NEBULISATION WITH DUOLIN &BUDECORT
DEATH SUMMARY:
55 YEAR OLD FEMALE K/C/O DM SINCE 3 YEARS ON OHAS WITH A/H/O GIDDINESS AND
HYPOTENSION @ OUTSIDE HOSPITAL FOLLOWING WHICH 10 NS GIVEN [NO
DOCUMENTATION AVAILABLE ],AFTER THAT PATIENT DEVELOPED FACIAL PUFFINESS
,PEDAL EDEMA ONE DAY AGO.
C/O LOOSE STOOLS 4-5 EPISODES SINCE 1 DAY ,BOWEL AND URINARY INCONTINENCE 4
TIMES SINCE 1 DAY ,NO C/O SEIZURES ,HEADACHE .
C/O ACUTE SOB GRADE 4 @ AROUND 4PM ON 10/5/22 AND UNRESPONSIVE SINCE 30
MINUTES.AT PRESENTATION PATIENT IS UNRESPONSIVE ,GCS-E1V1M1,SPO2-29@ ROOM
AIR,GRBS -331,BP-140/100MMHG,RR-26CPM.BILATERAL DIFFUSE WHEEZE PRESENT.
INJ LASIX 40MG ,NEBULISATIONS,HEAD END ELEVATION GIVEN ,SPO2 IMPROVED TO 90%
WITH HIGH FLOW 02,ABG WAS DONE WITH HIGH FLOW O2 -PH-6.846,PCO2-106MMHG,PO2-
108,SO2-93.1,HCO3-17.4,STHCO3-11.4,INJ NAHCO3 50MEQ IV STAT GIVEN FOLLOWED BY
100MEQ IN 100ML NS .PATIENT HAD SUDDEN CARDIAC ARREST AT 1.00AM ,CPR STARTED
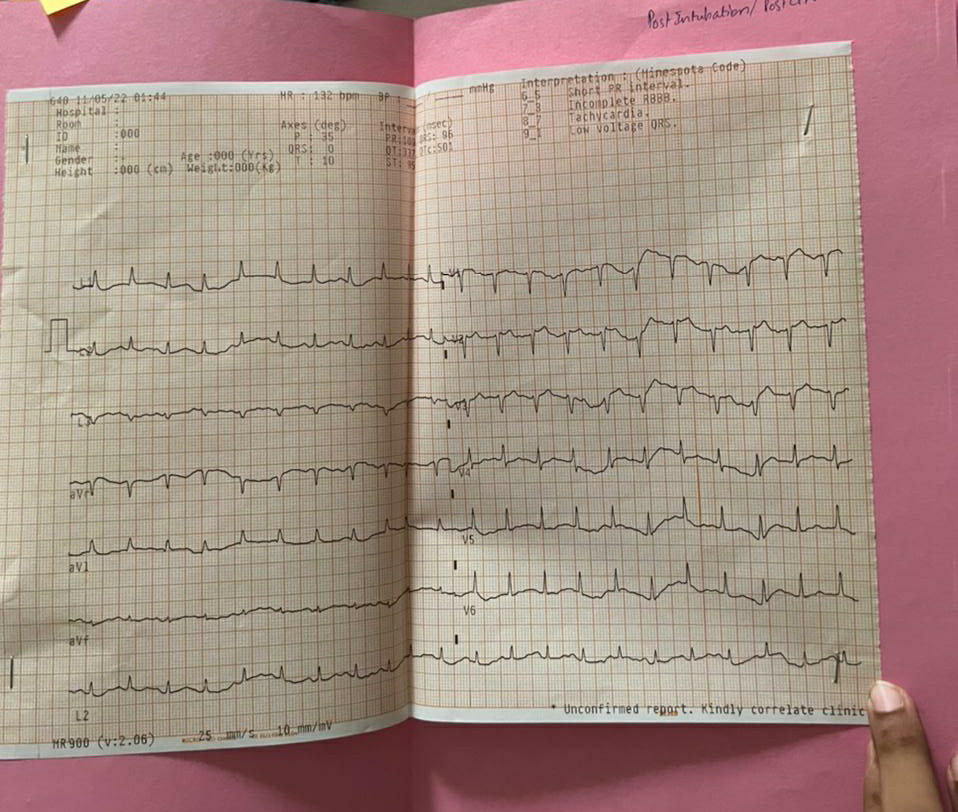
ACCORDING TOACCS GUIDELINES.AFTER 6 CYCLES OF CPR ROSC ATTAINED ,INTUBATED
AND CONNECTED TO MECHANICAL VENTILATOR .POST INTUBATION BP-NR,STARTED ON
INOTROPES.PATIENT HAD ANOTHER EPISODE OF SUDDEN CARDIAC ARREST @ 1.50AM.
AFTER 7 CYCLES OF CPR ROSC ATTAINED .BP-NR,PR-132BPM.PATIENT HAD ONE MORE
EPISODE OF SUDDEN CARDIAC ARREST AT 2.35AM ,AND 2 CYCLES OF CPR DONE .INSPITE
OF ALL ABOVE EFFORTS PATIENT COULD NOT BE REVIVED AND DECLARED DEAD ON
11/5/22 AT 2.45 AM
IMMEDIATE CAUSE OF DEATH : SUDDEN CARDIAC ARREST SECONDARY METABOLIC TO
SEVERE METABOLIC ACIDOSIS WITH TYPE 2 RESPIRATORY FAILURE
ANTECEDENT CAUSE OF DEATH : ACUTE GASTROENTERITIS WITH AKI ,MIXED ACIDOSIS ,?
HYPERCAPNIC ENCEPHALOPATHY
COMORBIDITIES: DIABETES MELLITUS



Comments
Post a Comment